An ambitious plan tailored to deliver coronavirus vaccines to California’s most vulnerable populations is fraying under pressure to simplify and speed up the state’s rocky vaccination rollout.
A week after Gov. Gavin Newsom expanded vaccine eligibility to residents 65 and older, state officials are now proposing a plan to complete vaccinations for all seniors before anyone else. The shift is causing frustration among health advocates who have spent the last two months hashing out a plan that prioritized essential workers and gave more weight to racial and socioeconomic factors.
With a scarce vaccine supply and a mounting death toll, the tension between equity and efficiency is increasing.
“The feedback that we got is, the first system is too complicated, it’s slowing us down,” said Tomás Aragón, the new director of the state’s Department of Public Health, who helped outline the new age-based priority proposal at public meetings on Jan. 12 and Jan. 20. “Got to keep it simple. Simplicity is going to save lives.”
Distributing vaccines by age is easier and will help ease the burden on the state’s overwhelmed health care system, Aragón said. Older people account for 65% of ICU admissions in California and 83% of deaths, according to the latest state health data.
But there are 6.2 million Californians 65 and older, and the state is only receiving up to 500,000 doses of vaccine every week, according to state epidemiologist Dr. Erica Pan. At that rate, the state wouldn’t begin vaccinating essential workers until May.
Disparate Impacts
Equity advocates called this proposed delay “disturbing,” arguing that many agricultural workers face equal or higher health risk at work than do elderly people who may have the means to shelter at home.
“Not everyone that’s 65 and over has the same level of vulnerability,” said Diana Tellefson Torres, executive director of the United Farm Workers Foundation. “Farmworkers are a very vulnerable population regardless of age.”
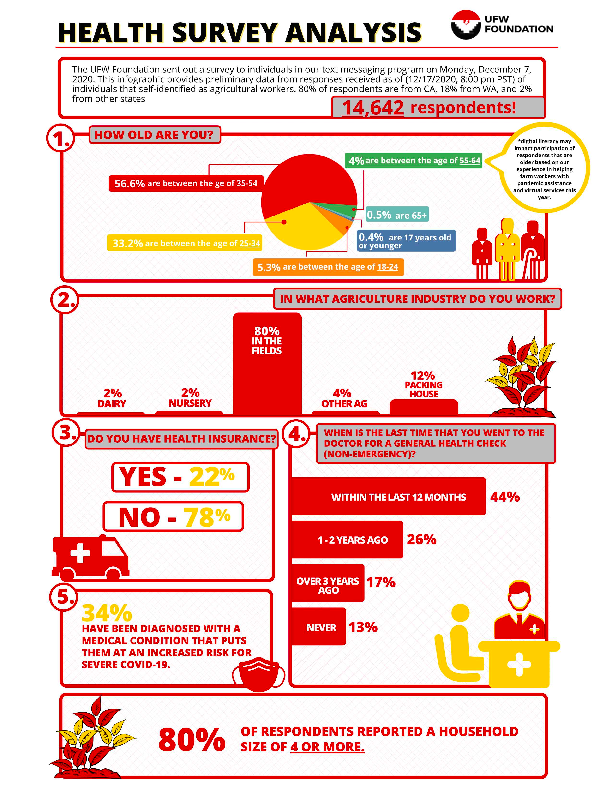
For example, 13% of agricultural workers have never been to a doctor and 78% do not have insurance, according to a UFW Foundation survey of 14,000 workers. Farmworkers, grocery store workers and meatpackers, who cannot work from home, have been disproportionately impacted by the coronavirus.
{kind=link}
It’s for those reasons the state initially placed food workers — along with teachers, emergency responders and people over 74 — next in line to get the vaccine after health care workers and residents and staff of long-term care homes. Some counties and employers had already notified these workers that they were next in line before the governor on Jan. 13 expanded eligibility to include people 65 and older.
“Moving millions of people farther ahead in line, by definition, means millions of others are farther back in line,” said Mitch Steiger, legislative advocate for the California Labor Federation.
Steiger’s group is one of 70 the state asked to be part of the Community Vaccine Advisory Committee to help develop a “safe, equitable, transparent” distribution plan. Many members saw it as an opportunity to correct some of the entrenched inequities in the health system, and even to repair historical injustices.
But now that counties and health providers are struggling with logistical challenges of administering the vaccine, some fault the committee’s work for being big on ideas but short on follow through.
“We have been so caught up in some of the minutia, honestly, of ‘What sectors? In which phase?’ ” said Denny Chan, senior staff attorney at Justice in Aging. “But we don’t seem to be spending the same amount of time and consideration on thinking through how you’re going to get to those people ultimately in the end.”
Logistics and Flexibility
Several members of the advisory group say moving to age-based priority guidelines will be a more efficient, effective means of administering scarce vaccines, while at the same time taking an equitable approach.
Health insurance plans say they have data on the age and underlying health conditions of their members and can easily notify them when they are eligible to receive the vaccine. But they don’t have reliable data on people’s occupations or job sectors.
“We know how to slice and dice the data to get to the populations that need it the most,” said Brianna Lierman, CEO of Local Health Plans of California, a trade group of insurers that cover low-income Medi-Cal patients. “Loosening it up so that we can get out there and get shots in people’s arms is absolutely the right thing to do.”
An age-based approach is one that is most likely to succeed and therefore can help build credibility with the public, Lierman said, adding, “A Medi-Cal lens is an equity lens.”
Some vaccine committee members are asking the state to give vaccinators more flexibility and discretion to help prevent doses from being wasted. That includes Mary McCune, regulatory affairs director with the California Dental Association, whose members are being tapped to help expand the state’s corps of vaccinators.
McCune said if there is someone like a farmworker who is 65 and has to drive an hour to a vaccination site with his wife, who’s 63, it makes sense to vaccinate them both at the same time, and maybe even their adult child who gave them a ride. That way, she added, you’re not asking each family member to travel back and forth three times before that person’s group is called.
This flexibility could also help overcome vaccine hesitancy in communities of color, said Kiran Savage-Sangwan, executive director of the California Pan-Ethnic Health Network.
Equity in an Age-Based System
After Newsom on Jan. 13 opened vaccinations to people 65 and older, seniors flooded phone lines and online registration portals, trying to get appointments at their doctors’ offices or one of the new mass-vaccination centers like those at Disneyland and Cal Expo. This overwhelmed existing health system infrastructure, and many seniors, at least those with the time and tenacity to wait it out, were left on hold for up to eight hours.
“The first-come, first-serve approach will inherently favor the people who are savvy enough to navigate those systems,” and many low-income or older seniors will be left out, said Chan, from Justice in Aging. “They’re going to require different strategies than the cookie-cutter, one-size-fits-all Dodger Stadium approach.”
A recent study investigating racial inequities in heart-failure treatment, showed white patients were more likely to receive specialty care because they were more likely to vigorously advocate for access to that care. Unless the state takes more proactive measures to reach vulnerable communities, the same trend will likely play out with vaccines, said Dr. Michelle Morse, a professor at Harvard Medical School who worked on the study.
“Folks who are white feel that they are entitled, or feel that they should have access to certain things that other groups have either been told that they shouldn’t have access to or actually have been intentionally excluded from having access to,” she said.
California health officials say they are aware of these trends and want to counteract them. They believe they can still pursue equity goals within an age-based system, said Dr. Nadine Burke-Harris, California’s surgeon general and co-chair of the vaccine committee.
The state, for example, is working on different ways to “operationalize equity,” she said. It is developing outreach strategies for vulnerable communities and may direct a certain percentage of vaccines to seniors in low-income neighborhoods based on the state’s Healthy Places Index, which measures access to safe housing, education and health care by ZIP code.
“This is a data-based tool to calculate how to distribute scarce resources equitably,” she said. “It supports a need for both simplicity and equity.”